Think salary is the most important component of total compensation for physicians? Think again. Today, the most common physician compensation model is a base salary plus a productivity bonus largely based on work Relative Value Units (wRVUs). Your workload, measured in wRVUs, impacts your paycheck more than anything else in many employment contracts. On Marit, approximately 40% of all physician salary contracts have productivity as a core component of total compensation. So whether you’re negotiating a new job or just trying to understand your current one, it’s crucial to grasp what wRVUs are, how they work, and how they vary across specialties.
What is a wRVU and Why Does It Matter?
A wRVU (work Relative Value Unit) is a standardized unit that quantifies the work a physician performs. Every patient encounter or procedure is assigned a wRVU value based on the time, complexity, skill, and effort typically required. For example, a basic 15-minute office visit (CPT code 99213) carries around 1.30 wRVUs, whereas a more complex 45-minute visit (99215) is about 2.80 wRVUs (source). Surgical and procedural codes have higher wRVUs reflecting greater time & complexity – e.g. a cataract surgery with CPT code 66982 is ~10.25 wRVUs. wRVUs are an attempt to standardize the “productivity” of physicians across different specialties & services.
wRVUs matter because they are the currency of physician productivity. Medicare and most private insurers use RVUs behind the scenes to determine payments for services (via the formula RVUs × conversion factor in dollars). More directly for physicians, hospitals and practices use wRVUs to measure your output against benchmarks. Compensation models often tie pay to wRVUs: either through bonuses for exceeding certain wRVU thresholds, or in pure productivity-based contracts that pay a set dollar amount per wRVU generated. Thus, your total annual wRVUs become a key metric of your performance and value to the organization. Knowing your wRVU totals and how they compare to norms is important for negotiating fair compensation and setting work expectations. See AAFP's overview on this topic here
How Do wRVU-Based Compensation Models Work?
In a wRVU-based compensation model, your income is directly linked to the wRVUs you produce. The simplest version is a pure productivity model: you get paid X dollars per wRVU, with no fixed base salary. For example, if a contract pays $45 per wRVU and you log 5,000 wRVUs in a year, you’d earn $225,000 (5,000 × $45, see here). Often, there are tiered incentives: e.g. $45 per wRVU for the first 5,000 wRVUs, then $50 per wRVU for any wRVUs beyond that, to reward higher productivity. Pure wRVU models (sometimes called “eat-what-you-kill”) are common in procedural specialties and private practices, comprising about 13% of contracts in Marit’s community-powered dataset.
Under any wRVU model, the critical component is the conversion factor, i.e. dollars paid per wRVU. This rate might be set based on national benchmarks (for example, MGMA or AMGA median $/wRVU for your specialty) and adjusted based on local market dynamics or individual negotiation. We’ll discuss typical $/wRVU rates by specialty in the next section. Physicians should always know their conversion rate and how it compares to benchmarks – it’s effectively your “price per unit” of work.
Additionally, clarity on what activities count toward wRVUs is important: generally, it’s only billable clinical services. Tasks like administrative meetings, teaching, or patient phone calls usually do not generate wRVUs (unless there are specific billing codes for them, which is rare), a drawback of pure RVU models. This means you could be working hard in other ways that don’t directly increase your wRVU tally. Some contracts provide separate stipends for non-clinical duties for this reason.
Finally, note that wRVU-based models rely on accurate coding, documentation, and tracking. If you under-code your visits or forget to bill a procedure, you’re leaving wRVUs (and thus money) on the table. Your employer's finance department should be tracking this data, and you should request to see them from time to time. If those reports aren’t provided, don’t hesitate to ask – it’s your productivity data and key to understanding your performance
wRVU Volume Benchmarks by Specialty
How many wRVUs do physicians typically produce in a year? It varies drastically by specialty. For example, a family medicine doctor seeing patients in clinic all day will accrue far fewer wRVUs than, say, a busy general surgeon or radiologist performing high-volume procedures.
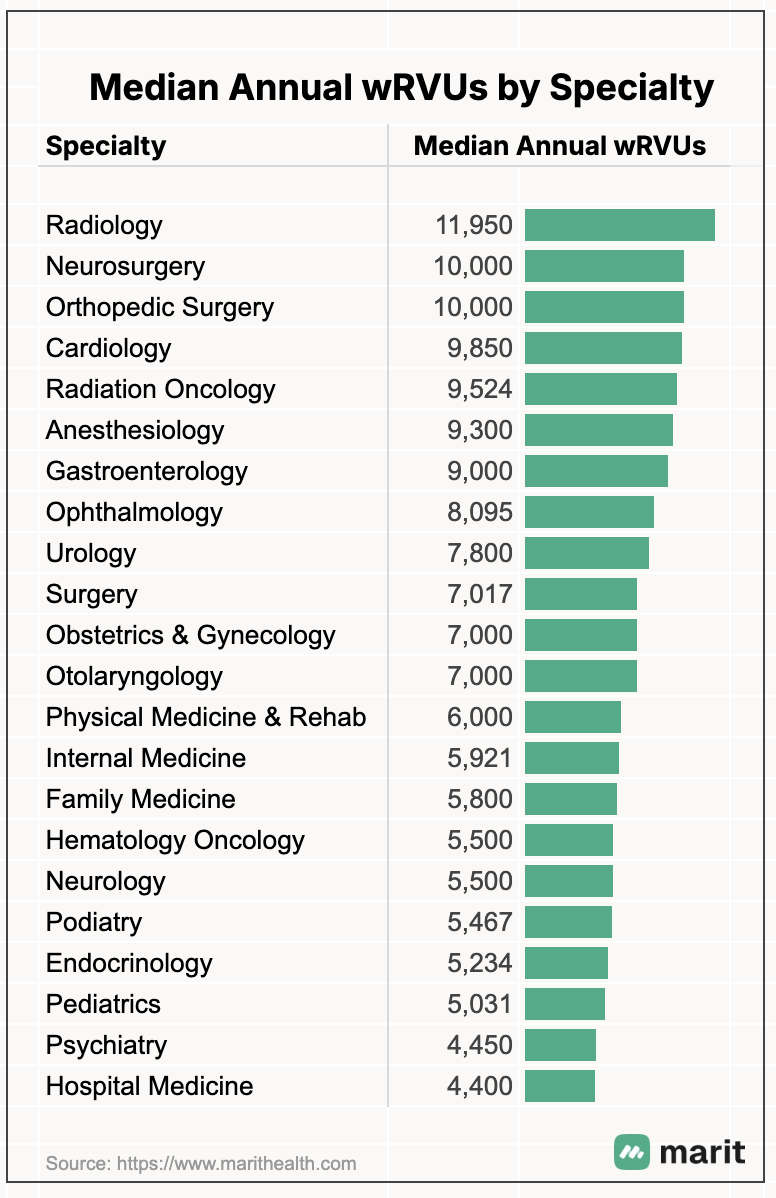
The chart above shows median wRVUs based on all doctor salary contributions on Marit. In primary care fields, e.g., family medicine, hospital medicine, pediatrics, etc. - median annual wRVUs are around 4,500 - 6,000 per full-time physician. In contrast, surgical and procedural specialties tend to generate much higher volumes – often on the order of 7,000 -10,000+ wRVUs per year on average. For instance, orthopedic surgeons generate a median of ~10,000 wRVUs, ~9,850 for cardiologists, and ~11,950 for radiologists.
But wRVUs is only one part of the story. To get the full picture, we also need to look at compensation per wRVU.
Compensation per wRVU ($/wRVU) Benchmarks by Specialty
“Compensation per wRVU” is the flip side of the coin – it’s the rate at which you’re paid for each wRVU. And it is the main important metric to negotiate in your contract. This metric (abbreviated as $/wRVU) effectively standardizes earnings relative to work output. It’s widely used for benchmarking and contract review. For example, if two gastroenterologists both earned $500,000 last year but one logged 10,000 wRVUs and the other 7,000 wRVUs, their comp per wRVU would be $50.0 and $71.4 respectively – a big difference.
$/wRVU is the most important metric to negotiate in your contract. Ultimately, your compensation will be directly tied to the $ conversion rate per wRVU
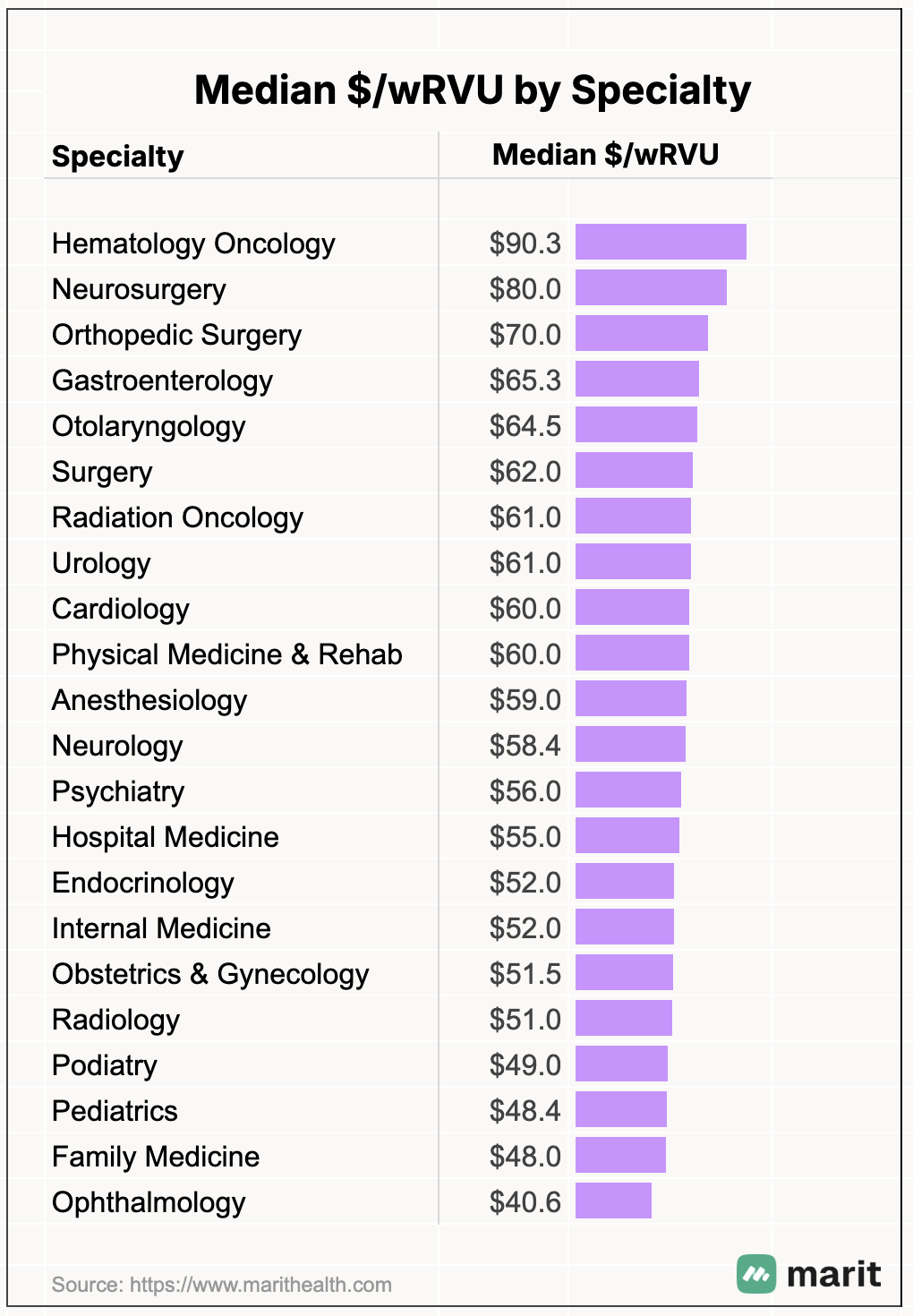
Much like wRVU volumes, there’s also significant variation in $/wRVU by specialty - ranging from $40 - $45 for Pediatrics or Ophthalmology to >$90 for Hematology Oncology. Why? Physicians who perform procedures generally generate significant additional income for their employers from facility fees, which is a common and much larger revenue stream for provider systems.
Below are the median $/wRVU by Specialty based on the physician salary data on Marit. Note that these are medians, and will vary by practice type, region, wRVU thresholds, etc. Much like salary, the more desirable the location, the less will be the $/wRVU reimbursement factor.
Ultimately the total annual compensation is the product of these two metrics - Annual wRVUs and $/wRVU. How do these two correlate? Turns out, there is a slight positive correlation (0.2) - i.e. specialties with high wRVUs also tend to have a higher reimbursement rate. Employers tend to compensate wRVUs generated from surgical specialists at a higher rate, thanks to the additional reimbursement they get from facility rates. This is a double-whammy - specialties like Pediatrics, Family Medicine, and Internal Medicine generate lower than average annual wRVUs and also get compensated at a lower $/wRVU. These specialties fall into the lower-left (purple) cluster.
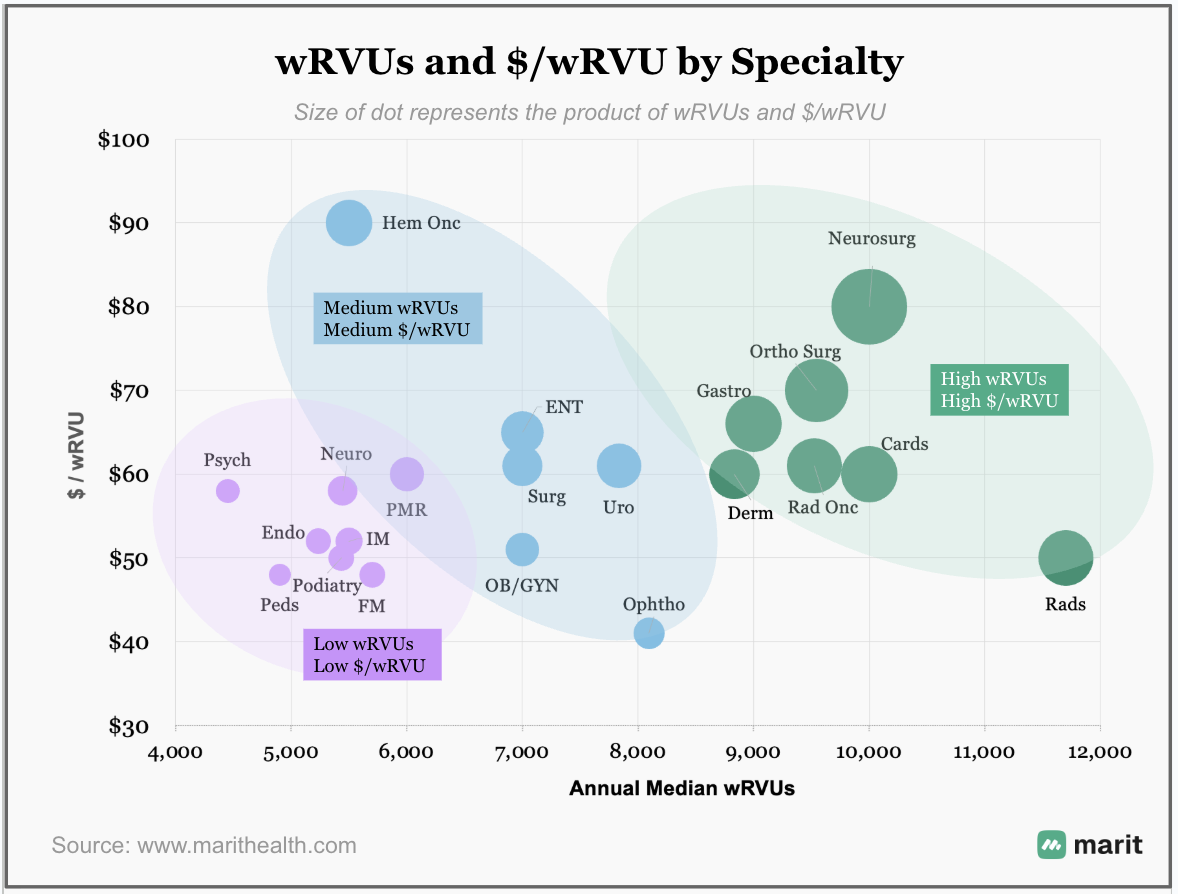
Specialties in the lower-left (purple) cluster – e.g. Pediatrics (Peds), Psychiatry (Psych), Endocrinology (Endo) – have relatively low wRVU totals and lower dollars per wRVU.
The middle (blue) cluster – e.g. Obstetrics/Gynecology (OB/GYN), General Surgery, Urology, ENT – represents moderate wRVUs and mid-range $/wRVU.
And the upper-right (green) cluster – e.g. Orthopedic Surgery (Ortho Surg), Neurosurgery, Radiology (Rads), Dermatology (Derm) – shows very high wRVU volumes coupled with higher $ per wRVU rates.
This variability in wRVU volume and $/wRVU reflects the wide disparities in compensation across different fields: a high-volume surgical sub-specialist can ultimately take home 3–4 times higher compensation than a Pediatrician.
Is your specialty missing?
We only calculated wRVU benchmarks for specialties where we had a large enough sample size to report meaningful data. Some specialties, especially smaller ones, or ones that are typically paid on non-productivity models, didn’t have enough submissions to meet that threshold.
If your specialty is missing, you can help change that.
👉 Sign up on Marit and share your salary anonymously. If you have already shared, please add your wRVU details here. And please invite your colleagues to do the same.
As more people contribute, we’ll be able to publish accurate data for more specialties, and together build the data-set we need to be able to advocate for ourselves.
How to Increase Your wRVUs (Boosting Productivity Ethically)
Unfortunately, medicare reimbursement rates per wRVU have steadily declined relative to inflation over the past 25 years, so in order to keep compensation simply on par with inflation, physicians need to generate more wRVUs each year.Here are some strategies physicians can use to boost wRVU productivity without just working longer hours or compromising quality:
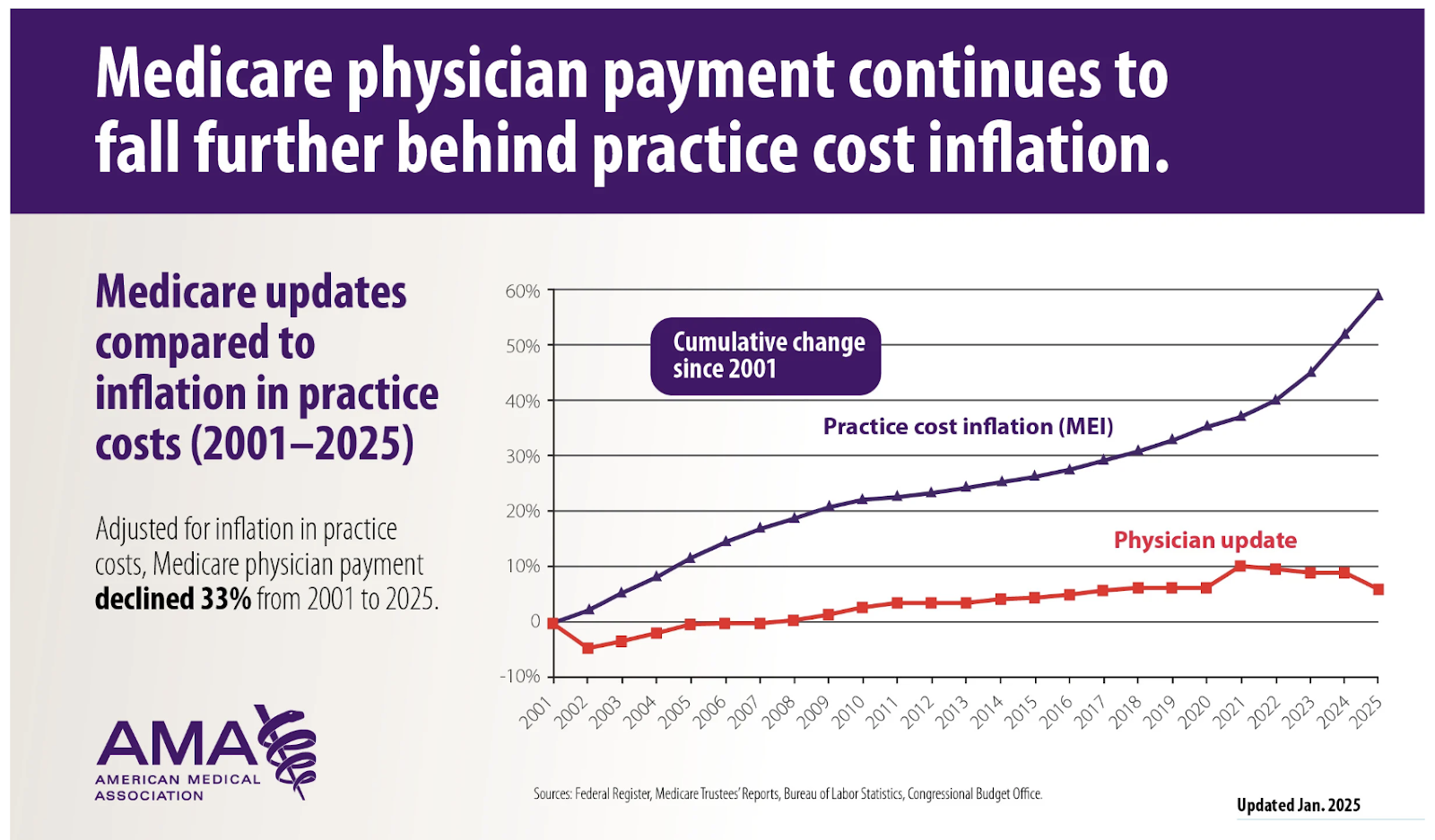
Source: CMS
- Improve Efficiency and Throughput: Optimize your workflow so you can see patients or do procedures more efficiently. This might involve streamlining documentation (e.g. using scribes or templates), delegating non-clinical tasks to support staff, and refining office scheduling to reduce no-shows or gaps. The more patients you can see in a day without extending hours, the more wRVUs you’ll accumulate.
- Optimize Coding and Documentation: Ensure you are capturing the full wRVUs for the work you already do. In practice, this means accurate coding at the appropriate levels. If you tend to under-code office visits (e.g. coding a 99213 when the encounter truly meets 99214), you’re losing RVUs.
- Manage Your Schedule Strategically: Pay attention to how your schedule is structured. For instance, filling cancellations promptly or double-booking certain slots (if no-show rates are high) can ensure your day stays full. Also, consider the balance of new patients vs follow-ups – new patient visits often have higher RVUs.
That said, please keep an eye on quality. It’s never worth sacrificing good patient care or burning yourself out just to chase a few extra RVUs. The only sustainable way of improving wRVUs comes down to seeing more patients (efficiently), coding better, and offering more high-value services – all within the scope of good care.
Conclusion
wRVUs have become a linchpin of compensation because they align payment with productivity in our healthcare system. They may seem confusing at first, but know your numbers – wRVUs generated, your compensation per wRVU, and how those compare to benchmarks. And be proactive in managing your time, coding, and services to ensure you’re capturing the full value of the care you deliver.
At Marit, we’re building a comprehensive salary resource to help you benchmark your RVU metrics, set appropriate expectations for you and your employer, and advocate for smarter contracts. If you haven’t contributed yet, please share your compensation and productivity data anonymously to help bring more transparency to medicine.
About the Data & Methodology
Marit's Data is different. It is -
Unique - since it captures the compensation data along with all the details that matter - bonuses, shifts, scheduls, benefits, and more
Comprehensive - Across all specialties and Professions (Physicians & APPs), Employer Types (large and small, including Self-employed, Academic & Non Academic), Job Types (Full Time, Part Time, PRNs and Locums) and Employment Types (W-2, 1099, K-1)
Current - Unlike other benchmarks that only update their data once a year, all salaries reflect the clinician’s current compensation, and all averages are updated in real-time as new salaries are added
All data in this report comes from anonymized salary contributions on Marit, as of Jul 1, 2025. Only verified salary reports approved by our moderation team are included.
Feedback?
If you have any suggestions or requests for customized analysis or topics of research - we'd love to hear from you.

Let's create the most accurate benchmarks